Research Peptides to Prescription Peptides: How Operators Survive the 2026 FDA Reclassification
Provider Network and Compliance
•

Research Peptides to Prescription Peptides: How Operators Survive the 2026 FDA Reclassification
Most operators selling peptides in 2026 think the FDA reclassification is good news for the research peptide market. The opposite is true. The same wave of regulatory action bringing peptides like BPC-157 and Thymosin Alpha-1 back into legal compounding is also closing the gray market that supplied them for the last five years.
The window for operating in either lane is closing fast. By the end of 2026, two types of peptide businesses will be left standing. Brands and clinics with a legitimate prescription pathway through a licensed compounding pharmacy, and brands and clinics that have shut down. There will not be much in between.
This article walks through what actually happened with the FDA's Category 2 reclassification, why the research peptide era is ending regardless, how the revenue math changes under a prescription model, and what every operator selling peptides needs in place before the July 2026 Pharmacy Compounding Advisory Committee meeting. It introduces the Prescription Pathway Stack, the four-pillar framework Healthaide uses to evaluate whether a partner clinic or brand is ready to launch a compliant peptide program.
What Actually Happened with the FDA Peptide Reclassification
On February 27, 2026, HHS Secretary Robert F. Kennedy Jr. announced that roughly 14 of the 19 peptides previously placed on the FDA's Category 2 restricted compounding list would move back toward Category 1. The reversal followed two years of advocacy from medical providers, compounding pharmacy groups, and the broader functional medicine community (Pharmacy Times, "The Peptide Reclassification Everyone's Talking About," June 2026).
On April 15, 2026, twelve peptides were officially removed from Category 2. The list includes BPC-157, TB-500, Thymosin Alpha-1, Ipamorelin, CJC-1295, AOD-9604, GHK-Cu, Selank, Semax, KPV, MOTS-C, and several others.
Here is the part most of the headlines got wrong. Removal from Category 2 is not the same as clearance to compound. The FDA's bulk drug substances framework requires a substance to sit on the 503A authorized bulks list before licensed pharmacies can legally prepare it. Until that happens, the practical compounding status for patients and clinicians has not changed. The Pharmacy Compounding Advisory Committee meets on July 23 and 24, 2026, to review whether the removed peptides should be added to that list. The earliest legal compounding access could resume is late in the third quarter of 2026, and only with a favorable committee vote followed by FDA action (Pharmacy Times, June 2026).

A handful of peptides, including Melanotan II, GHRP-2, GHRP-6, and PEG-MGF, are expected to stay restricted because of ongoing safety concerns.
For operators, the takeaway is simple. The peptides that powered the gray market are coming back, but only through a regulated prescription pathway. The unregulated middle is gone.
Why the Research Peptide Era Is Ending Regardless
The reclassification is dominating headlines, but it is not the most important story for operators. The bigger shift is happening on the enforcement side, and it has been building for more than a year.
Between mid-2025 and early 2026, the research peptide industry lost more vendors than in the previous five years combined. The founders of Amino Asylum, one of the largest gray-market research compound stores in the country, pleaded guilty to federal charges on December 10, 2025, after investigators found that products labeled as SARMs actually contained testosterone, a controlled substance. That case followed the Tailor Made Compounding prosecution, which ended in a $1.79 million forfeiture.
The FDA's enforcement footprint reaches well beyond peptides. On March 3, 2026, the agency issued 30 warning letters to telehealth companies for making false or misleading claims about compounded GLP-1 products. The primary violations were implying sameness with FDA-approved products and obscuring the actual source of compounded drugs (FDA, "FDA Warns 30 Telehealth Companies Against Illegal Marketing of Compounded GLP-1s," March 2026).
That action came after a September 2025 crackdown on direct-to-consumer pharmaceutical advertising. In six months, the FDA sent more warning letters than it had in the entire preceding decade (FDA, March 2026).
The clearest signal came on February 6, 2026, when HHS General Counsel Mike Stuart announced that Hims and Hers Health had been referred to the Department of Justice for investigation tied to its compounded GLP-1 practices (Telehealth.org, "FDA Warns Telehealth Firms Over Compounded GLP-1," March 2026).
Every one of these actions rests on the same principle. Compounded medications, peptides included, must be prepared by licensed pharmacies under a physician's prescription, with real clinical oversight. Mass-marketed, transactional, gray-market models are no longer treated as a regulatory gray area. They are treated as enforcement targets.
If you are currently selling research peptides under a "for research use only" label, or relying on a 503A pharmacy operating outside its scope, the message is hard to miss. That business model has expired.
The Prescription Pathway Stack: What You Need to Sell Peptides Legally in 2026
This is the framework we use to evaluate whether a clinic, brand, or operator is ready to launch a compliant peptide program. Four pillars. All four have to be in place. Miss one and the whole thing is exposed.
Pillar One: A Licensed Prescribing Provider in Each Patient's State
Every prescription peptide has to be issued by a physician or qualified mid-level provider actively licensed in the state where the patient lives. This is the requirement operators underestimate most. A physician licensed only in Texas cannot supervise a prescription for a patient in Florida. Adding a telehealth interface does not remove that rule. It multiplies it across every state your patients live in.
For a multi-state operation, that means either contracting providers licensed in every one of those states, or working with a managed provider network like Healthaide Medical Group P.C., led by Dr. Russell Van Maele, D.O., which already holds active licensure across all 50 states. Building state-by-state coverage on your own takes months. A managed network is live on day one.
Pillar Two: A 503A or 503B Compounding Pharmacy Partnership
Once Category 1 status is restored after the July meeting, the peptides still have to come from a properly licensed compounding pharmacy. The difference between 503A and 503B matters more than most operators realize.
A 503A pharmacy compounds patient-specific prescriptions. Each dose is prepared in response to one prescription for one patient. A 503B outsourcing facility prepares larger sterile batches that a clinic can stock as office inventory. Both are FDA-regulated. They serve different use cases and carry different requirements.
Operators sourcing from unlicensed labs, overseas suppliers, or research-grade vendors are not just taking on compliance risk. They are taking on product liability that no insurance policy will cover when something goes wrong.
Pillar Three: An EMR with Documented Good Faith Exam Workflows
Every prescription requires documentation. That documentation includes a good faith examination, defined by the state where the patient lives, completed before the prescription is written. The good faith exam is not paperwork for its own sake. It is the legal foundation that makes the prescription valid in the first place.
State medical boards in New York, California, Texas, and Florida have all disciplined telehealth-only prescribers, and they are looking specifically at whether contraindication screening and informed consent happened in the same visit as the prescription. An operator running peptide intake through a generic CRM or a 30-second web form is not running a compliant program. They are building a liability event with a delayed trigger. The American Med Spa Association puts it plainly. Charts must show what service was performed, who supervised it, and the clinical reasoning behind it (American Med Spa Association, 2025).
A platform like Healthaide folds the EMR, intake, good faith exam workflow, and prescription routing into one system, so compliance is part of how the program runs rather than something stapled on afterward.
Pillar Four: A Compliant Product Menu That Respects FDA Enforcement Priorities
Not every peptide on the old Category 2 list is coming back. Building a 2026 peptide menu means knowing which compounds will be available through legal compounding after July, which will stay restricted, and how to describe each one in marketing without stepping into the exact territory the FDA is enforcing against.
Copy that implies sameness with FDA-approved drugs, references brand names in misleading ways, or promises specific clinical outcomes is precisely what the March 2026 warning letters targeted (FDA, March 2026). A compliant menu starts with verified peptides, accurate descriptions, no FDA-approval implications, no outcome guarantees, and pricing that reflects a supervised medical model instead of an ecommerce checkout.
How Does the Revenue Math Change Under Prescription Peptides?
Operators who built businesses around research-grade peptides usually assume the prescription model is less profitable. Run the numbers across a full year of a patient relationship and the assumption falls apart.
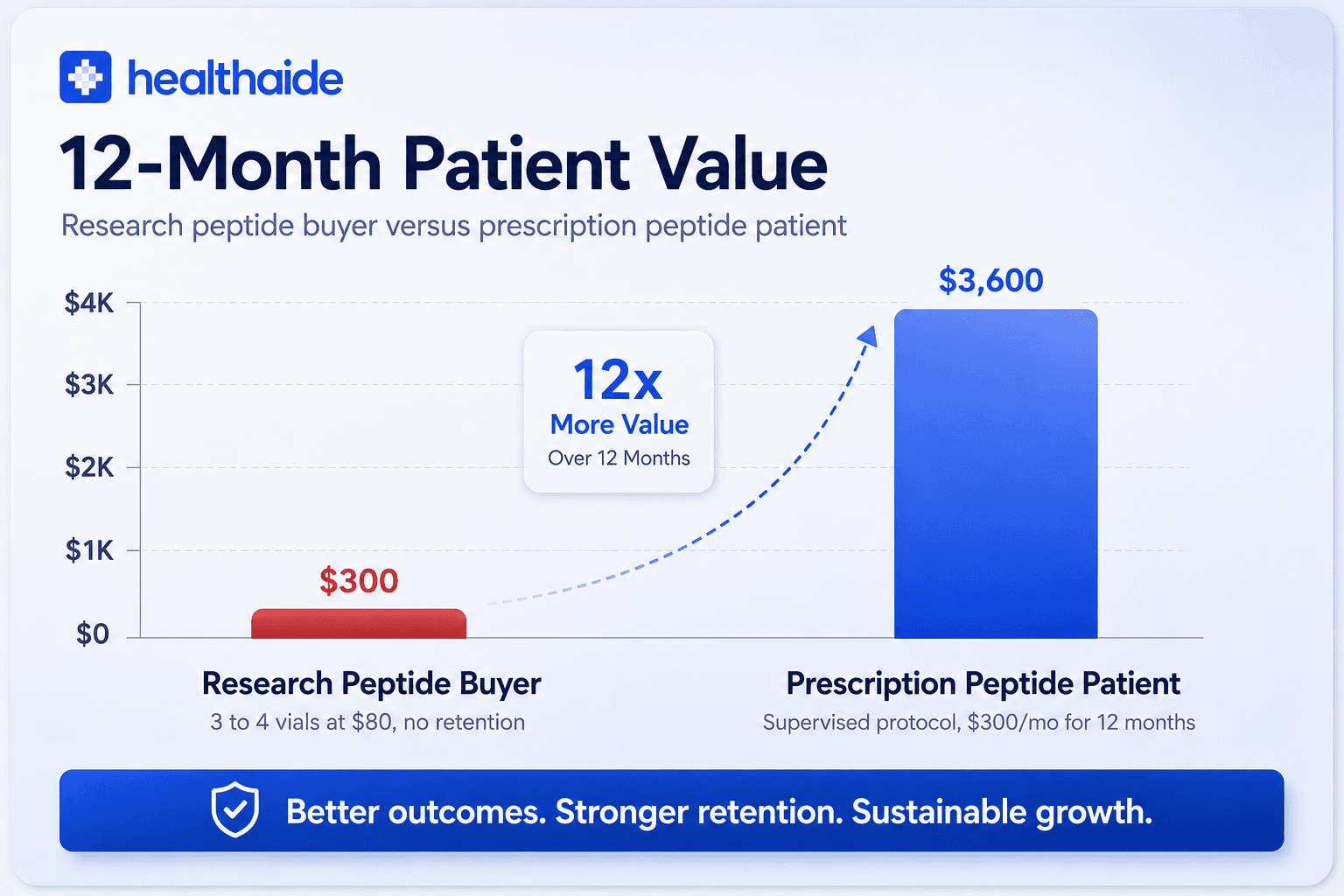
A gray-market operator selling BPC-157 at $80 for a 5mg vial, with no supervision, earns about $80 per transaction. The buyer typically picks up three or four vials before churning to whoever is cheaper next month, which works out to roughly $250 to $320 in lifetime revenue. Margin after sourcing sits around 40 to 50 percent, and acquisition costs run high because trust is thin and reorders are unpredictable.
A prescription-pathway operator selling the same compound inside a supervised six-month protocol prices it at $300 to $400 per month, including the consult, the prescription, and the medication. Retention is far higher because the program includes monitoring, dose adjustments, and integration with other services the patient already wants. Annual revenue per patient lands somewhere between $2,400 and $4,800. Margin holds up because the model supports premium pricing.
A prescription peptide patient is worth roughly ten to fifteen times more than a research peptide buyer over twelve months. The prescription model also produces something the gray market never could. Compliant marketing, lower legal exposure, and a defensible position the next time enforcement letters go out.
The gray market was never the profitable choice. It was the easy one.
What Mistakes Are Operators Making Right Now?
Five mistakes keep showing up as operators try to navigate the reclassification window.
The first is waiting until July to make any decisions. Operators are watching the PCAC meeting like it will answer everything. It will answer which peptides can be compounded. It will not answer a single infrastructure question. The provider network, the pharmacy partnership, the EMR, and the documentation workflows all take weeks to build. Whoever waits until late Q3 to start will be half a year behind whoever is building now.
The second is running two pathways at once. Some operators are keeping research peptide sales alive while quietly building a prescription pathway alongside it. This is a gift to enforcement attorneys. Any documented evidence that you were selling research peptides to consumers undermines your good faith position later. The dual pathway is more dangerous than either pathway on its own.
The third is sourcing from compounding pharmacies that may not survive the current environment. Not every 503A pharmacy operating today will still be operating in twelve months. The FDA has been sending warning letters to compounders that marketed compounded GLP-1 products as equivalent to approved drugs. Source from a pharmacy under active scrutiny and you inherit that scrutiny by association.
The fourth is treating the good faith exam as a checkbox. It is the legal spine of the entire pathway. Boards are auditing for it specifically. An operator using a quick intake form and calling it an exam is sitting in the same crosshairs as the GLP-1 telehealth platforms that got the March letters.
The fifth is marketing peptides like a supplement brand. Calling them research-grade, posting before-and-after photos without medical context, implying weight loss guarantees, or name-dropping FDA-approved drugs without disclosure are the exact patterns the FDA has been targeting. A prescription peptide program is medical care, and the marketing has to read like it.
What Should Wellness Brands and Med Spas Do Before July 2026?
The PCAC meeting is weeks away. For an operator who has not yet built a prescription pathway, a realistic timeline looks like this.
In the next two weeks, audit your current peptide sourcing. If you are selling research-grade peptides to consumers, stop. The downside scenarios are severe. If you are buying compounded peptides from a pharmacy you cannot fully verify, request licensure documentation and FDA registration confirmation. If they cannot produce it immediately, find a different pharmacy.
In the next four weeks, stand up provider coverage in every state where your patients live. If you have customers in 30 states, you need provider licensure in 30 states. The two practical routes are contracting providers state by state or partnering with a managed network. The second is faster, cheaper, and lower risk for most operators.
In the next six weeks, put an EMR in place with an integrated good faith exam workflow, intake documentation, and prescription routing. It needs to capture clinical reasoning, contraindications, lab work where indicated, and patient consent, and it needs to retain those records for as long as each state's rules require.
In the next eight weeks, rewrite every piece of marketing on your site, in your ads, and in your email sequences. Strip out FDA-approval implications, misleading brand-name references, and outcome guarantees. Replace them with accurate, medically responsible descriptions of what peptide therapy is and is not.
This is the work that separates the operators running compliant peptide programs in the fourth quarter from the operators shutting their doors.
FAQ
Are peptides like BPC-157 legal in 2026? Not yet through compounding pharmacies, even after the April 2026 reclassification. The FDA removed BPC-157 from the Category 2 restricted list on April 15, 2026, but compounding pharmacies still cannot legally prepare it until the Pharmacy Compounding Advisory Committee votes to add it to the 503A authorized bulks list. That vote is scheduled for July 23 and 24, 2026. The earliest legal compounding access could resume is late in the third quarter of 2026, pending a favorable vote and FDA follow-through.
What is the difference between research peptides and prescription peptides? Research peptides are sold for laboratory and scientific research only, not for human consumption, and do not require a prescription. Prescription peptides are compounded by a licensed pharmacy for a specific patient under a physician's prescription, with required clinical oversight, documentation, and a good faith examination. Selling research peptides for human use is illegal no matter how the products are labeled.
Do I need a medical director to legally offer peptide therapy? You need a licensed prescribing provider, which can be an employed medical director, a contracted physician, or a managed provider network like Healthaide Medical Group P.C. The provider has to hold active licensure in every state where patients live and must complete a good faith examination before issuing any prescription.
How does the FDA peptide reclassification affect telehealth platforms? Telehealth platforms selling peptides now operate in the same enforcement environment as the GLP-1 telehealth companies that received 30 FDA warning letters in March 2026. The standards for marketing claims, prescribing practices, and pharmacy sourcing are identical. Platforms that cannot show physician oversight, state licensure compliance, and legitimate pharmacy partnerships are exposed.
What happens to operators who keep selling research peptides after the PCAC meeting? Federal enforcement against research peptide vendors has accelerated sharply, with multiple criminal prosecutions in 2025 and 2026, including the Amino Asylum and Tailor Made Compounding cases. The risk profile for any operator continuing to sell research-grade peptides to consumers has climbed and is expected to keep climbing.
The Operators Who Survive 2026 Are Building Infrastructure, Not Watching Headlines
The peptide reclassification will be remembered as the moment the wellness industry split into two groups. The operators who treated compliance as the foundation of a real business will own the prescription peptide market for the next decade. The ones who treated it as friction will not be in the market at all.
The infrastructure question stopped being theoretical the day the first warning letters went out. It is now the line between being in business in January 2027 and watching from the sidelines.
If you are working out how to build a compliant prescription peptide program, book a demo at healthaide.io/demo to see how operators are launching with full provider coverage, pharmacy fulfillment, and EMR infrastructure in under 30 days. The full platform overview is at healthaide.io/features, and pricing is at healthaide.io/pricing.
References
U.S. Food and Drug Administration, "FDA Warns 30 Telehealth Companies Against Illegal Marketing of Compounded GLP-1s," March 3, 2026. https://www.fda.gov/news-events/press-announcements/fda-warns-30-telehealth-companies-against-illegal-marketing-compounded-glp-1s
Pharmacy Times, "The Peptide Reclassification Everyone's Talking About: A Pharmacist's Take on What RFK Jr's Announcement Actually Means," June 2026. https://www.pharmacytimes.com/view/the-peptide-reclassification-everyone-s-talking-about-a-pharmacist-s-take-on-what-rfk-jr-s-announcement-actually-means
American Med Spa Association, "FDA Targets Telehealth Compounded GLP-1 Marketing in New Warning Letters," March 6, 2026. https://americanmedspa.org/news/fda-targets-telehealth-compounded-glp-1-marketing-in-new-warning-letters
American Med Spa Association, "Physician Supervision: Keeping the Medical in Medical Spas," 2025. https://americanmedspa.org/blog/physician-supervision-keeping-the-medical-in-medical-spas
Telehealth.org, "FDA Warns Telehealth Firms Over Compounded GLP-1," March 17, 2026. https://telehealth.org/news/fda-warns-telehealth-companies-over-marketing-of-compounded-glp-1-weight-loss-drugs/
KFF Health News, "Telehealth Booms as Demand for GLP-1s Surges and Questions Mount About Safety, Oversight," June 2026. https://kffhealthnews.org/health-industry/glp1-weight-loss-drugs-telehealth-oversight-regulation-compounded-semaglutide/
Related insights


Research Peptides to Prescription Peptides: How Operators Survive the 2026 FDA Reclassification
Provider Network and Compliance
•
Research Peptides to Prescription Peptides: How Operators Survive the 2026 FDA Reclassification
Most operators selling peptides in 2026 think the FDA reclassification is good news for the research peptide market. The opposite is true. The same wave of regulatory action bringing peptides like BPC-157 and Thymosin Alpha-1 back into legal compounding is also closing the gray market that supplied them for the last five years.
The window for operating in either lane is closing fast. By the end of 2026, two types of peptide businesses will be left standing. Brands and clinics with a legitimate prescription pathway through a licensed compounding pharmacy, and brands and clinics that have shut down. There will not be much in between.
This article walks through what actually happened with the FDA's Category 2 reclassification, why the research peptide era is ending regardless, how the revenue math changes under a prescription model, and what every operator selling peptides needs in place before the July 2026 Pharmacy Compounding Advisory Committee meeting. It introduces the Prescription Pathway Stack, the four-pillar framework Healthaide uses to evaluate whether a partner clinic or brand is ready to launch a compliant peptide program.
What Actually Happened with the FDA Peptide Reclassification
On February 27, 2026, HHS Secretary Robert F. Kennedy Jr. announced that roughly 14 of the 19 peptides previously placed on the FDA's Category 2 restricted compounding list would move back toward Category 1. The reversal followed two years of advocacy from medical providers, compounding pharmacy groups, and the broader functional medicine community (Pharmacy Times, "The Peptide Reclassification Everyone's Talking About," June 2026).
On April 15, 2026, twelve peptides were officially removed from Category 2. The list includes BPC-157, TB-500, Thymosin Alpha-1, Ipamorelin, CJC-1295, AOD-9604, GHK-Cu, Selank, Semax, KPV, MOTS-C, and several others.
Here is the part most of the headlines got wrong. Removal from Category 2 is not the same as clearance to compound. The FDA's bulk drug substances framework requires a substance to sit on the 503A authorized bulks list before licensed pharmacies can legally prepare it. Until that happens, the practical compounding status for patients and clinicians has not changed. The Pharmacy Compounding Advisory Committee meets on July 23 and 24, 2026, to review whether the removed peptides should be added to that list. The earliest legal compounding access could resume is late in the third quarter of 2026, and only with a favorable committee vote followed by FDA action (Pharmacy Times, June 2026).
A handful of peptides, including Melanotan II, GHRP-2, GHRP-6, and PEG-MGF, are expected to stay restricted because of ongoing safety concerns.
For operators, the takeaway is simple. The peptides that powered the gray market are coming back, but only through a regulated prescription pathway. The unregulated middle is gone.
Why the Research Peptide Era Is Ending Regardless
The reclassification is dominating headlines, but it is not the most important story for operators. The bigger shift is happening on the enforcement side, and it has been building for more than a year.
Between mid-2025 and early 2026, the research peptide industry lost more vendors than in the previous five years combined. The founders of Amino Asylum, one of the largest gray-market research compound stores in the country, pleaded guilty to federal charges on December 10, 2025, after investigators found that products labeled as SARMs actually contained testosterone, a controlled substance. That case followed the Tailor Made Compounding prosecution, which ended in a $1.79 million forfeiture.
The FDA's enforcement footprint reaches well beyond peptides. On March 3, 2026, the agency issued 30 warning letters to telehealth companies for making false or misleading claims about compounded GLP-1 products. The primary violations were implying sameness with FDA-approved products and obscuring the actual source of compounded drugs (FDA, "FDA Warns 30 Telehealth Companies Against Illegal Marketing of Compounded GLP-1s," March 2026).
That action came after a September 2025 crackdown on direct-to-consumer pharmaceutical advertising. In six months, the FDA sent more warning letters than it had in the entire preceding decade (FDA, March 2026).
The clearest signal came on February 6, 2026, when HHS General Counsel Mike Stuart announced that Hims and Hers Health had been referred to the Department of Justice for investigation tied to its compounded GLP-1 practices (Telehealth.org, "FDA Warns Telehealth Firms Over Compounded GLP-1," March 2026).
Every one of these actions rests on the same principle. Compounded medications, peptides included, must be prepared by licensed pharmacies under a physician's prescription, with real clinical oversight. Mass-marketed, transactional, gray-market models are no longer treated as a regulatory gray area. They are treated as enforcement targets.
If you are currently selling research peptides under a "for research use only" label, or relying on a 503A pharmacy operating outside its scope, the message is hard to miss. That business model has expired.
The Prescription Pathway Stack: What You Need to Sell Peptides Legally in 2026
This is the framework we use to evaluate whether a clinic, brand, or operator is ready to launch a compliant peptide program. Four pillars. All four have to be in place. Miss one and the whole thing is exposed.
Pillar One: A Licensed Prescribing Provider in Each Patient's State
Every prescription peptide has to be issued by a physician or qualified mid-level provider actively licensed in the state where the patient lives. This is the requirement operators underestimate most. A physician licensed only in Texas cannot supervise a prescription for a patient in Florida. Adding a telehealth interface does not remove that rule. It multiplies it across every state your patients live in.
For a multi-state operation, that means either contracting providers licensed in every one of those states, or working with a managed provider network like Healthaide Medical Group P.C., led by Dr. Russell Van Maele, D.O., which already holds active licensure across all 50 states. Building state-by-state coverage on your own takes months. A managed network is live on day one.
Pillar Two: A 503A or 503B Compounding Pharmacy Partnership
Once Category 1 status is restored after the July meeting, the peptides still have to come from a properly licensed compounding pharmacy. The difference between 503A and 503B matters more than most operators realize.
A 503A pharmacy compounds patient-specific prescriptions. Each dose is prepared in response to one prescription for one patient. A 503B outsourcing facility prepares larger sterile batches that a clinic can stock as office inventory. Both are FDA-regulated. They serve different use cases and carry different requirements.
Operators sourcing from unlicensed labs, overseas suppliers, or research-grade vendors are not just taking on compliance risk. They are taking on product liability that no insurance policy will cover when something goes wrong.
Pillar Three: An EMR with Documented Good Faith Exam Workflows
Every prescription requires documentation. That documentation includes a good faith examination, defined by the state where the patient lives, completed before the prescription is written. The good faith exam is not paperwork for its own sake. It is the legal foundation that makes the prescription valid in the first place.
State medical boards in New York, California, Texas, and Florida have all disciplined telehealth-only prescribers, and they are looking specifically at whether contraindication screening and informed consent happened in the same visit as the prescription. An operator running peptide intake through a generic CRM or a 30-second web form is not running a compliant program. They are building a liability event with a delayed trigger. The American Med Spa Association puts it plainly. Charts must show what service was performed, who supervised it, and the clinical reasoning behind it (American Med Spa Association, 2025).
A platform like Healthaide folds the EMR, intake, good faith exam workflow, and prescription routing into one system, so compliance is part of how the program runs rather than something stapled on afterward.
Pillar Four: A Compliant Product Menu That Respects FDA Enforcement Priorities
Not every peptide on the old Category 2 list is coming back. Building a 2026 peptide menu means knowing which compounds will be available through legal compounding after July, which will stay restricted, and how to describe each one in marketing without stepping into the exact territory the FDA is enforcing against.
Copy that implies sameness with FDA-approved drugs, references brand names in misleading ways, or promises specific clinical outcomes is precisely what the March 2026 warning letters targeted (FDA, March 2026). A compliant menu starts with verified peptides, accurate descriptions, no FDA-approval implications, no outcome guarantees, and pricing that reflects a supervised medical model instead of an ecommerce checkout.
How Does the Revenue Math Change Under Prescription Peptides?
Operators who built businesses around research-grade peptides usually assume the prescription model is less profitable. Run the numbers across a full year of a patient relationship and the assumption falls apart.
A gray-market operator selling BPC-157 at $80 for a 5mg vial, with no supervision, earns about $80 per transaction. The buyer typically picks up three or four vials before churning to whoever is cheaper next month, which works out to roughly $250 to $320 in lifetime revenue. Margin after sourcing sits around 40 to 50 percent, and acquisition costs run high because trust is thin and reorders are unpredictable.
A prescription-pathway operator selling the same compound inside a supervised six-month protocol prices it at $300 to $400 per month, including the consult, the prescription, and the medication. Retention is far higher because the program includes monitoring, dose adjustments, and integration with other services the patient already wants. Annual revenue per patient lands somewhere between $2,400 and $4,800. Margin holds up because the model supports premium pricing.
A prescription peptide patient is worth roughly ten to fifteen times more than a research peptide buyer over twelve months. The prescription model also produces something the gray market never could. Compliant marketing, lower legal exposure, and a defensible position the next time enforcement letters go out.
The gray market was never the profitable choice. It was the easy one.
What Mistakes Are Operators Making Right Now?
Five mistakes keep showing up as operators try to navigate the reclassification window.
The first is waiting until July to make any decisions. Operators are watching the PCAC meeting like it will answer everything. It will answer which peptides can be compounded. It will not answer a single infrastructure question. The provider network, the pharmacy partnership, the EMR, and the documentation workflows all take weeks to build. Whoever waits until late Q3 to start will be half a year behind whoever is building now.
The second is running two pathways at once. Some operators are keeping research peptide sales alive while quietly building a prescription pathway alongside it. This is a gift to enforcement attorneys. Any documented evidence that you were selling research peptides to consumers undermines your good faith position later. The dual pathway is more dangerous than either pathway on its own.
The third is sourcing from compounding pharmacies that may not survive the current environment. Not every 503A pharmacy operating today will still be operating in twelve months. The FDA has been sending warning letters to compounders that marketed compounded GLP-1 products as equivalent to approved drugs. Source from a pharmacy under active scrutiny and you inherit that scrutiny by association.
The fourth is treating the good faith exam as a checkbox. It is the legal spine of the entire pathway. Boards are auditing for it specifically. An operator using a quick intake form and calling it an exam is sitting in the same crosshairs as the GLP-1 telehealth platforms that got the March letters.
The fifth is marketing peptides like a supplement brand. Calling them research-grade, posting before-and-after photos without medical context, implying weight loss guarantees, or name-dropping FDA-approved drugs without disclosure are the exact patterns the FDA has been targeting. A prescription peptide program is medical care, and the marketing has to read like it.
What Should Wellness Brands and Med Spas Do Before July 2026?
The PCAC meeting is weeks away. For an operator who has not yet built a prescription pathway, a realistic timeline looks like this.
In the next two weeks, audit your current peptide sourcing. If you are selling research-grade peptides to consumers, stop. The downside scenarios are severe. If you are buying compounded peptides from a pharmacy you cannot fully verify, request licensure documentation and FDA registration confirmation. If they cannot produce it immediately, find a different pharmacy.
In the next four weeks, stand up provider coverage in every state where your patients live. If you have customers in 30 states, you need provider licensure in 30 states. The two practical routes are contracting providers state by state or partnering with a managed network. The second is faster, cheaper, and lower risk for most operators.
In the next six weeks, put an EMR in place with an integrated good faith exam workflow, intake documentation, and prescription routing. It needs to capture clinical reasoning, contraindications, lab work where indicated, and patient consent, and it needs to retain those records for as long as each state's rules require.
In the next eight weeks, rewrite every piece of marketing on your site, in your ads, and in your email sequences. Strip out FDA-approval implications, misleading brand-name references, and outcome guarantees. Replace them with accurate, medically responsible descriptions of what peptide therapy is and is not.
This is the work that separates the operators running compliant peptide programs in the fourth quarter from the operators shutting their doors.
FAQ
Are peptides like BPC-157 legal in 2026? Not yet through compounding pharmacies, even after the April 2026 reclassification. The FDA removed BPC-157 from the Category 2 restricted list on April 15, 2026, but compounding pharmacies still cannot legally prepare it until the Pharmacy Compounding Advisory Committee votes to add it to the 503A authorized bulks list. That vote is scheduled for July 23 and 24, 2026. The earliest legal compounding access could resume is late in the third quarter of 2026, pending a favorable vote and FDA follow-through.
What is the difference between research peptides and prescription peptides? Research peptides are sold for laboratory and scientific research only, not for human consumption, and do not require a prescription. Prescription peptides are compounded by a licensed pharmacy for a specific patient under a physician's prescription, with required clinical oversight, documentation, and a good faith examination. Selling research peptides for human use is illegal no matter how the products are labeled.
Do I need a medical director to legally offer peptide therapy? You need a licensed prescribing provider, which can be an employed medical director, a contracted physician, or a managed provider network like Healthaide Medical Group P.C. The provider has to hold active licensure in every state where patients live and must complete a good faith examination before issuing any prescription.
How does the FDA peptide reclassification affect telehealth platforms? Telehealth platforms selling peptides now operate in the same enforcement environment as the GLP-1 telehealth companies that received 30 FDA warning letters in March 2026. The standards for marketing claims, prescribing practices, and pharmacy sourcing are identical. Platforms that cannot show physician oversight, state licensure compliance, and legitimate pharmacy partnerships are exposed.
What happens to operators who keep selling research peptides after the PCAC meeting? Federal enforcement against research peptide vendors has accelerated sharply, with multiple criminal prosecutions in 2025 and 2026, including the Amino Asylum and Tailor Made Compounding cases. The risk profile for any operator continuing to sell research-grade peptides to consumers has climbed and is expected to keep climbing.
The Operators Who Survive 2026 Are Building Infrastructure, Not Watching Headlines
The peptide reclassification will be remembered as the moment the wellness industry split into two groups. The operators who treated compliance as the foundation of a real business will own the prescription peptide market for the next decade. The ones who treated it as friction will not be in the market at all.
The infrastructure question stopped being theoretical the day the first warning letters went out. It is now the line between being in business in January 2027 and watching from the sidelines.
If you are working out how to build a compliant prescription peptide program, book a demo at healthaide.io/demo to see how operators are launching with full provider coverage, pharmacy fulfillment, and EMR infrastructure in under 30 days. The full platform overview is at healthaide.io/features, and pricing is at healthaide.io/pricing.
References
U.S. Food and Drug Administration, "FDA Warns 30 Telehealth Companies Against Illegal Marketing of Compounded GLP-1s," March 3, 2026. https://www.fda.gov/news-events/press-announcements/fda-warns-30-telehealth-companies-against-illegal-marketing-compounded-glp-1s
Pharmacy Times, "The Peptide Reclassification Everyone's Talking About: A Pharmacist's Take on What RFK Jr's Announcement Actually Means," June 2026. https://www.pharmacytimes.com/view/the-peptide-reclassification-everyone-s-talking-about-a-pharmacist-s-take-on-what-rfk-jr-s-announcement-actually-means
American Med Spa Association, "FDA Targets Telehealth Compounded GLP-1 Marketing in New Warning Letters," March 6, 2026. https://americanmedspa.org/news/fda-targets-telehealth-compounded-glp-1-marketing-in-new-warning-letters
American Med Spa Association, "Physician Supervision: Keeping the Medical in Medical Spas," 2025. https://americanmedspa.org/blog/physician-supervision-keeping-the-medical-in-medical-spas
Telehealth.org, "FDA Warns Telehealth Firms Over Compounded GLP-1," March 17, 2026. https://telehealth.org/news/fda-warns-telehealth-companies-over-marketing-of-compounded-glp-1-weight-loss-drugs/
KFF Health News, "Telehealth Booms as Demand for GLP-1s Surges and Questions Mount About Safety, Oversight," June 2026. https://kffhealthnews.org/health-industry/glp1-weight-loss-drugs-telehealth-oversight-regulation-compounded-semaglutide/